The Problem
Clinical guidelines designed for print,
not for the point of care.
150 NHS clinical guidelines exist as dense Word documents and PDFs, pages of tightly formatted text, complex decision flowcharts, manual drug-dosing equations, and tables that require scrolling across on a phone screen. Clinicians need answers in seconds. The original formats were not designed for that reality.
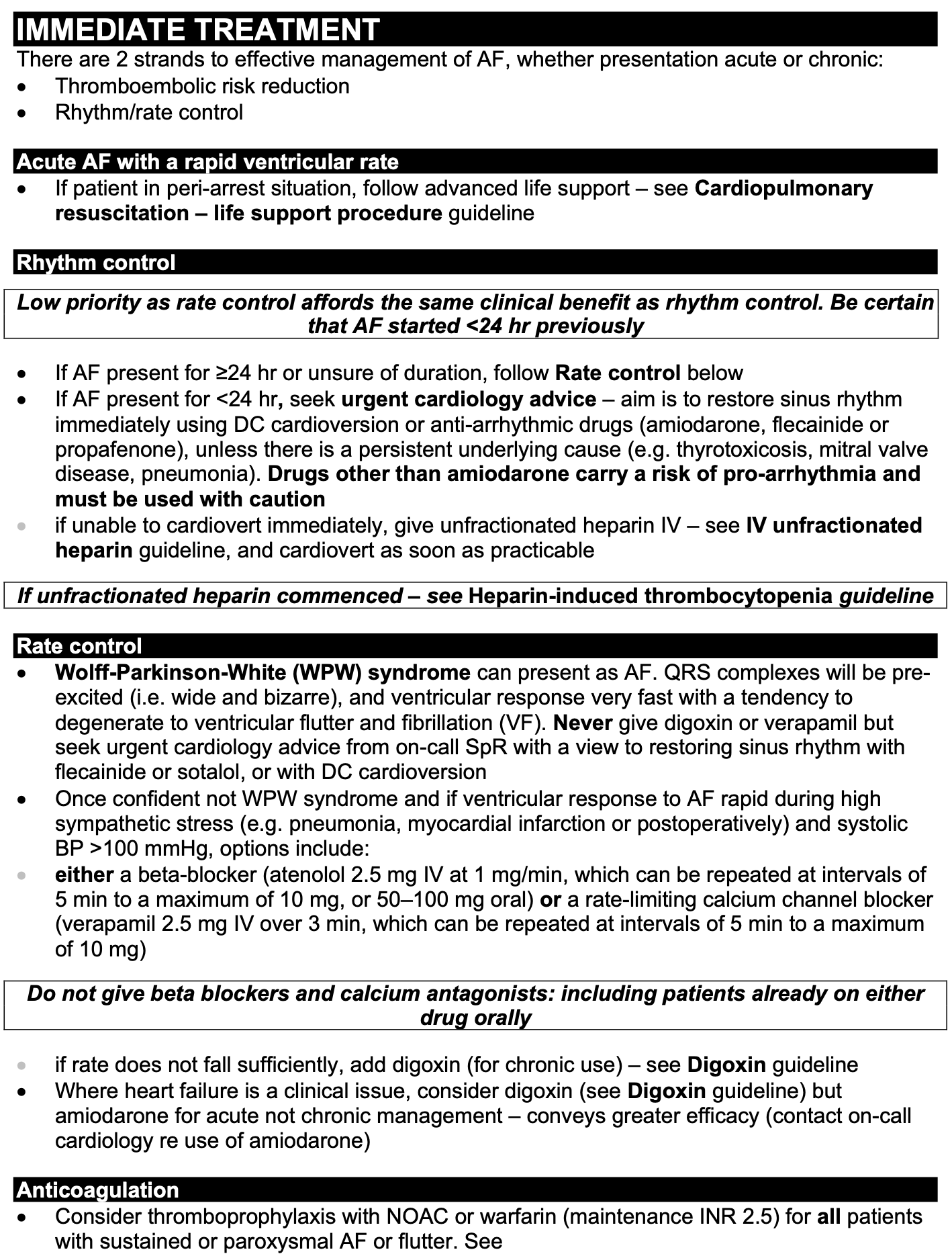
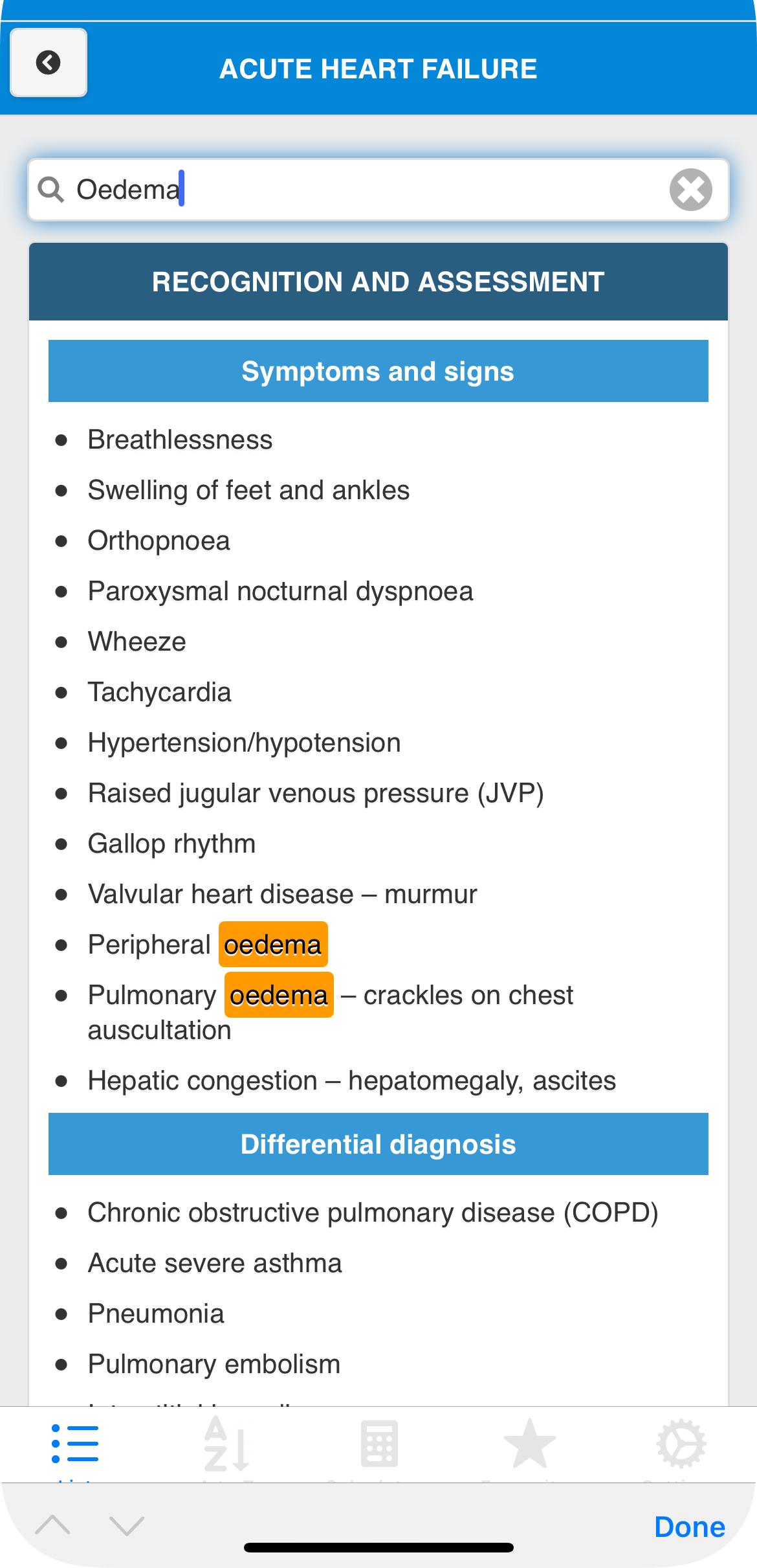
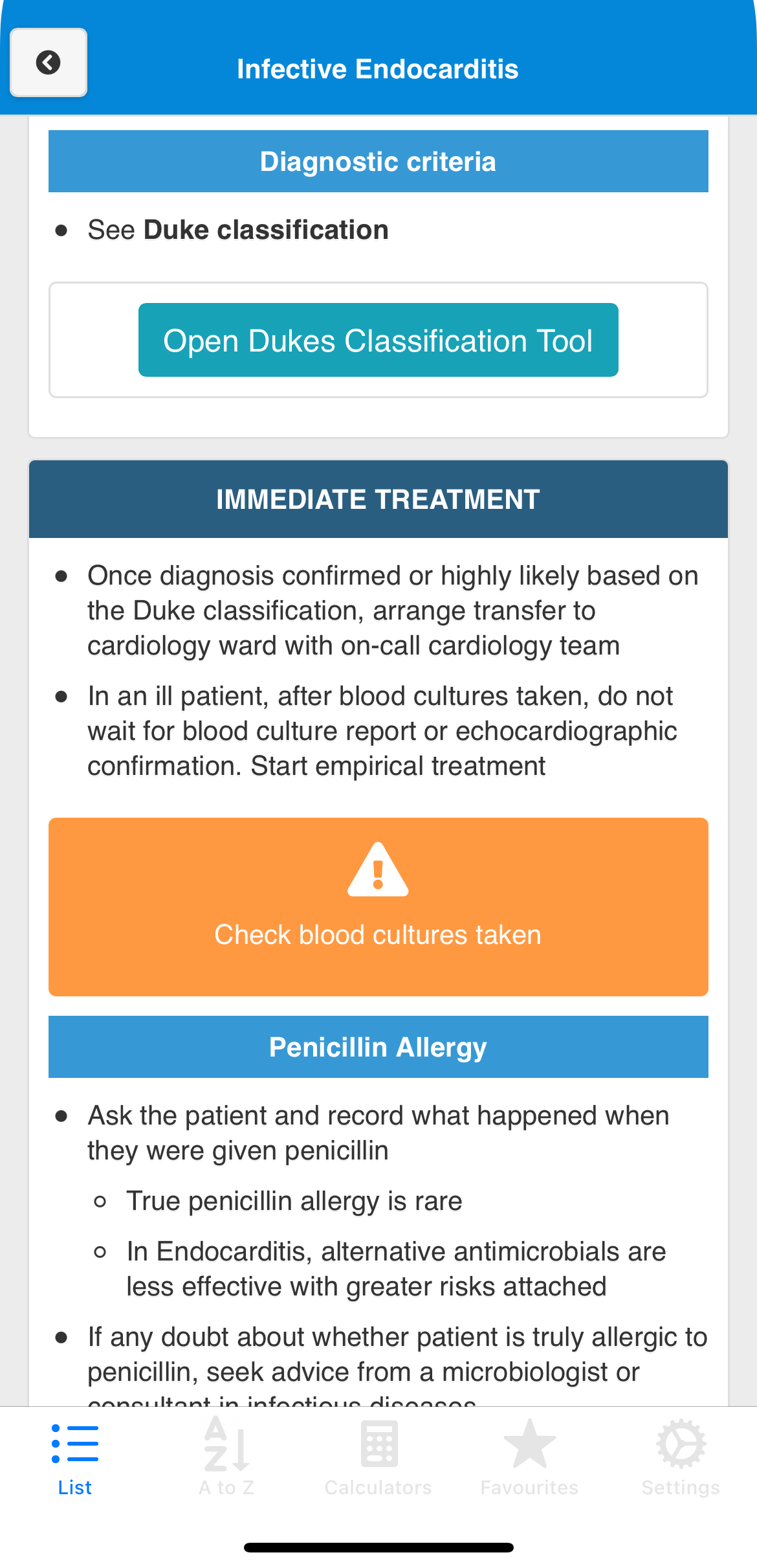
Atrial Fibrillation, wall of dense clinical text, complex bold/italic formatting, and multi-level bullets that require careful reading, not scanning.
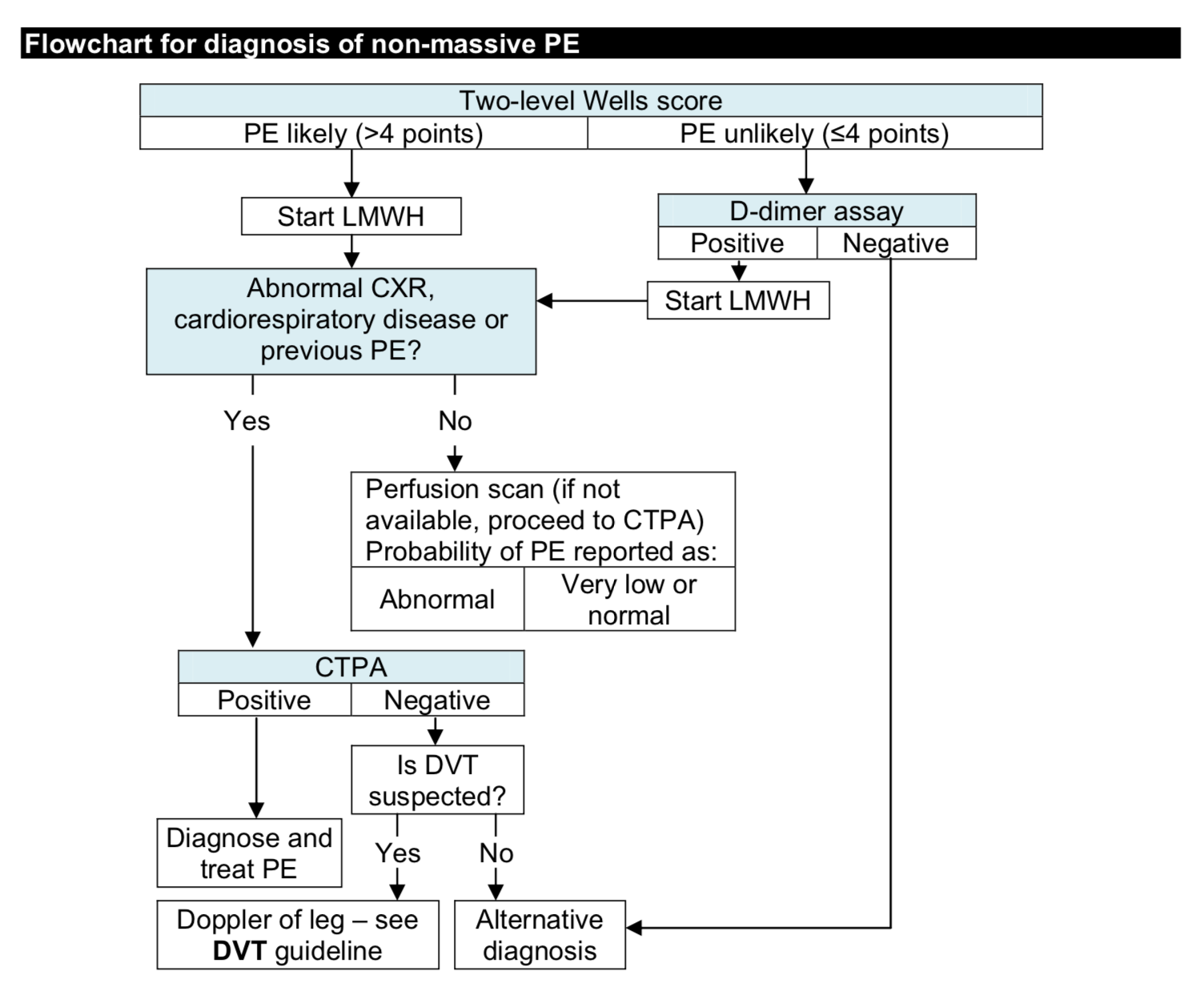
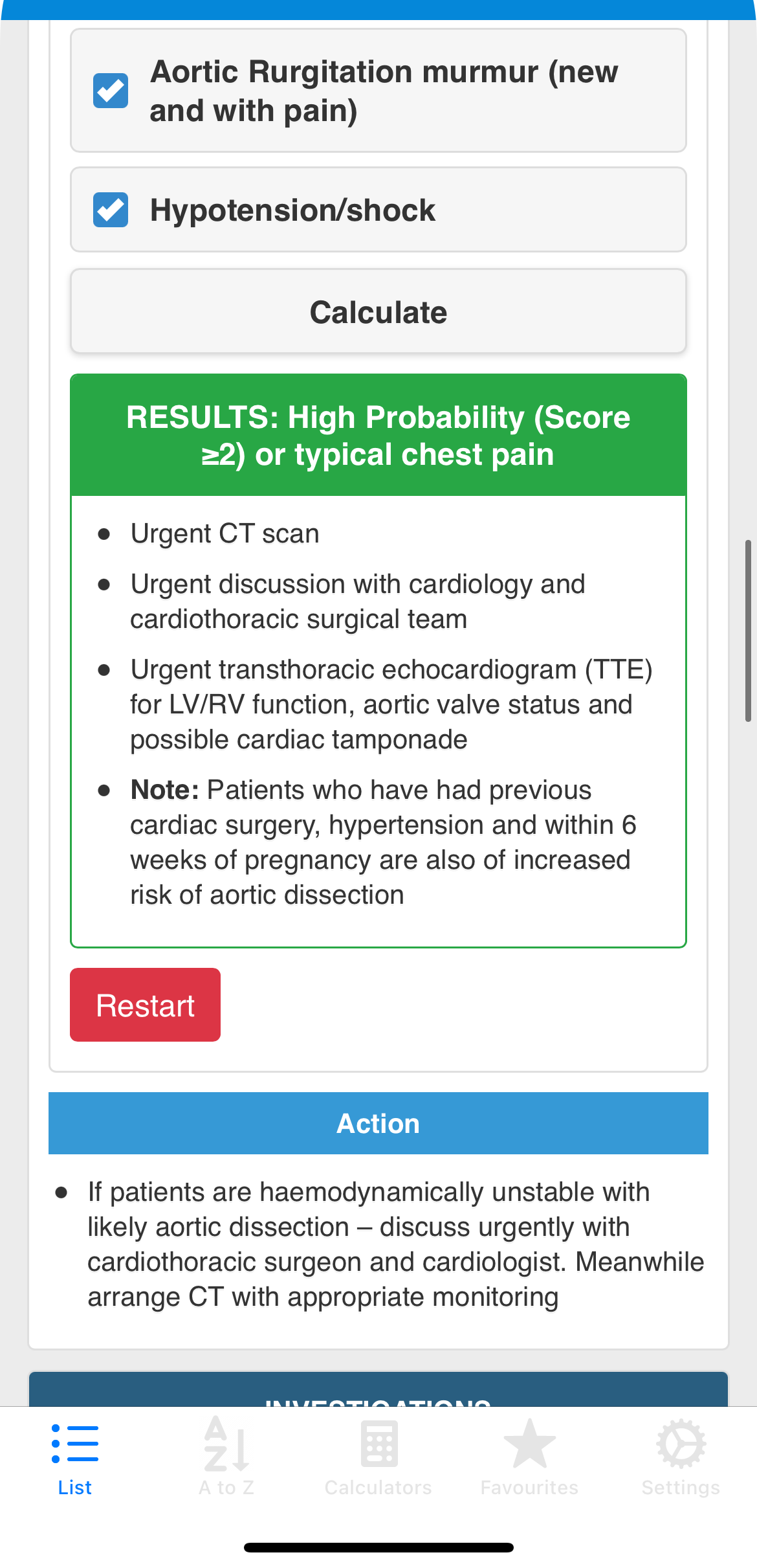
Pulmonary Embolism diagnosis, a complex branching flowchart impossible to follow on a mobile screen under ward conditions.
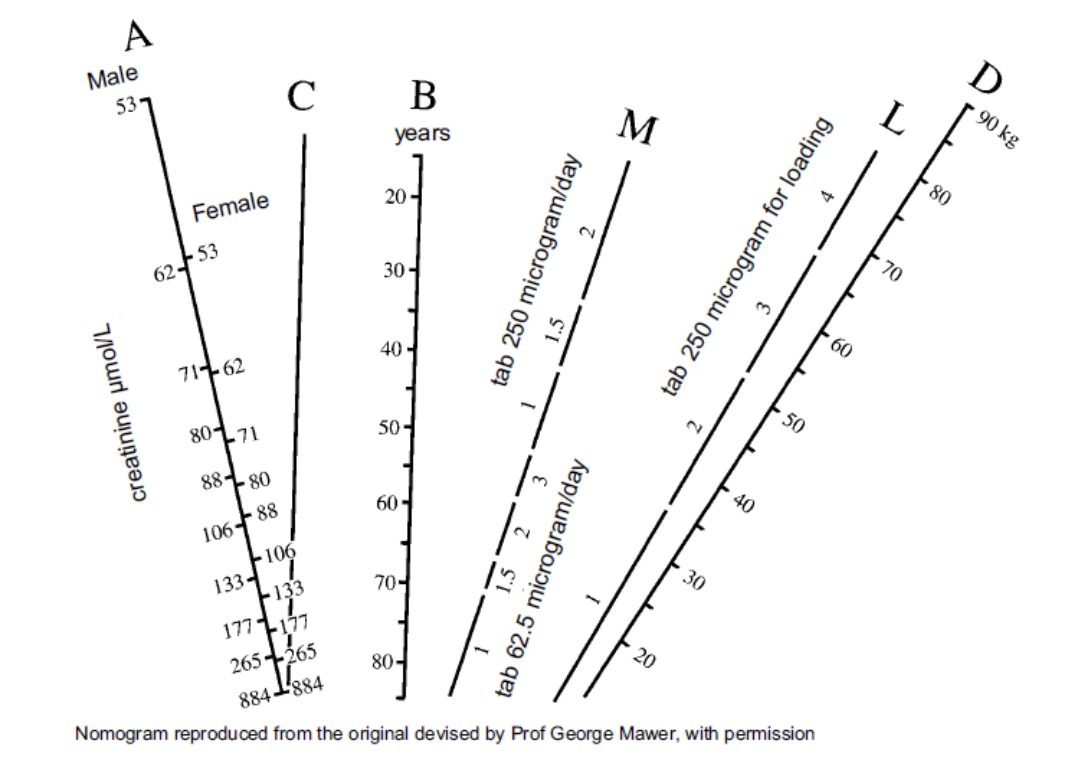
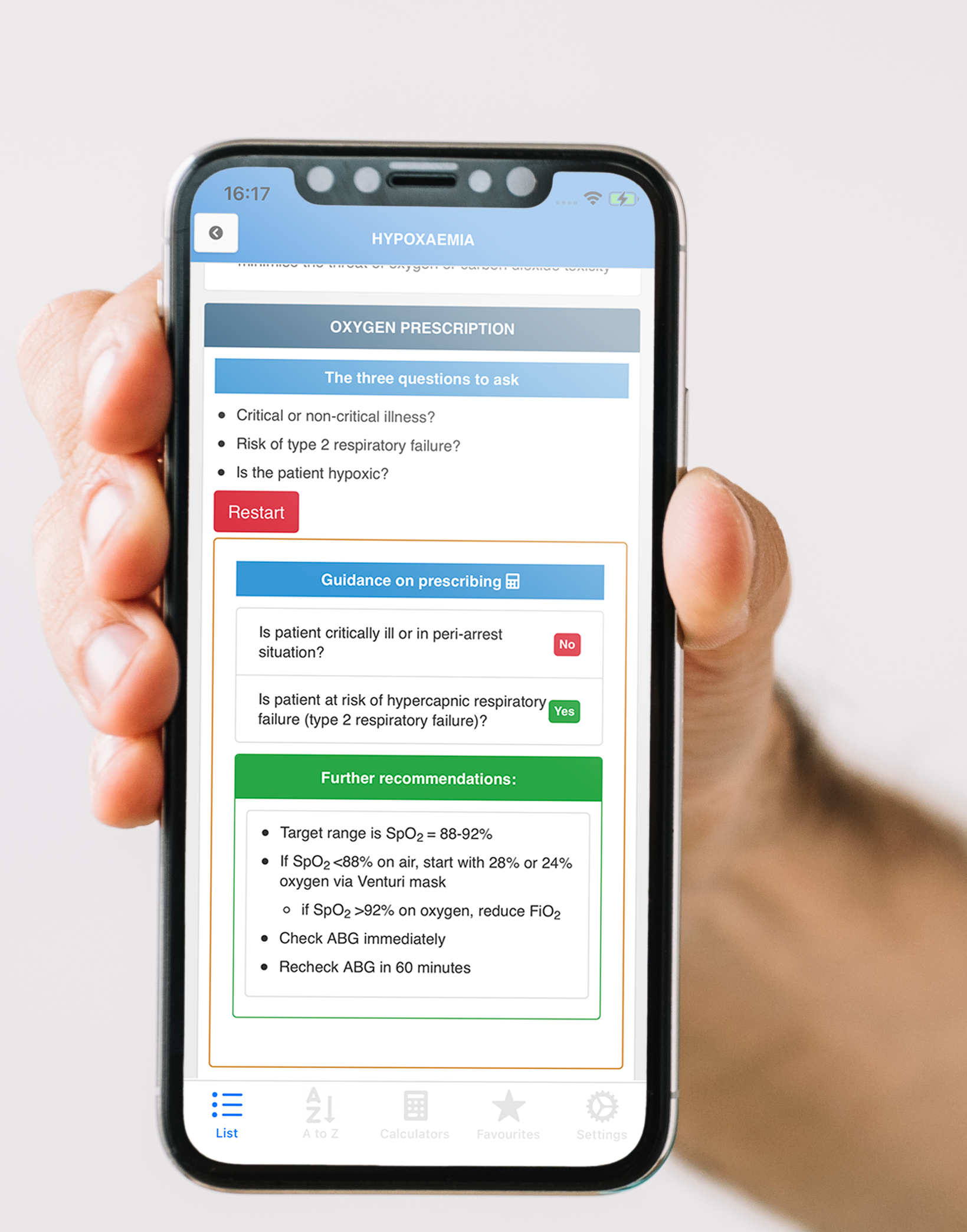
Gentamicin dosing, a nomogram requiring manual calculation using ruler and pencil interpolation, performed under time pressure at the bedside.
The Solution
Not a digital PDF. A rethink from the ward outwards.
This project began as Dr. Mitchell's PhD at Keele University, in close collaboration with University Hospital North Midlands NHS Trust. Working alongside respiratory physicians, nurses, and junior doctors through contextual inquiry and iterative usability evaluation, every design decision was shaped by observed clinical behaviour, not assumed needs.
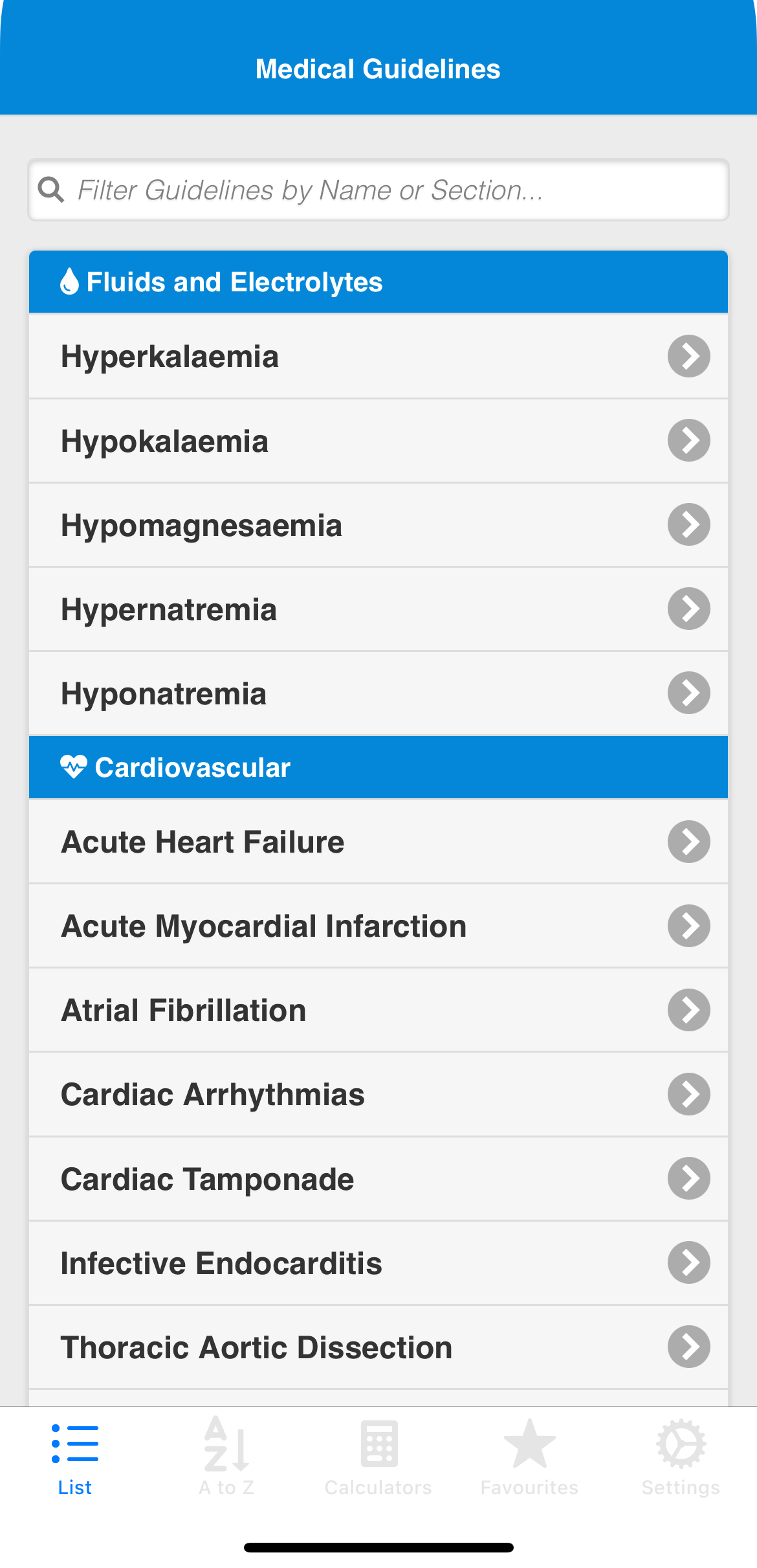
The result was the Bedside Clinical Guidelines (BCG) iOS app, 150 guidelines restructured into a two-tier visual hierarchy, with inline calculators, embedded decision tools, and a co-designed warning system. Deployed within UHNM NHS Trust, evaluated across five published studies, and producing 15 peer-reviewed design recommendations.
150
Guidelines
5
Papers
NHS
Deployed